Rugby is amongst the most played and watched sports in the world. The game is physically demanding, with bouts of walking, jogging, and running, interspersed with sprinting, static exertions, and contact events. Therefore, injuries are common in rugby and rugby shoulder injuries make up around 20% of all rugby injuries.
Most common rugby injuries in the shoulder affect the following structures:
Soft tissue around the shoulder
The shoulder complex, which consists of the clavicle, scapula, and humerus, connects the upper extremity to the thorax by a carefully crafted arrangement of three joints- the glenohumeral, acromioclavicular, and sternoclavicular. The articular structures of the shoulder complex are largely intended for mobility, enabling us to move and position the hand within a large range of space.
While being a primary joint responsible for the movement of the upper limb, stability is very important for the joint. Passive stabilization is provided by the bony architecture, the ligaments, the capsule, and the labrum. Additionally, muscles around the shoulder complex also provide dynamic stabilization to the joints.
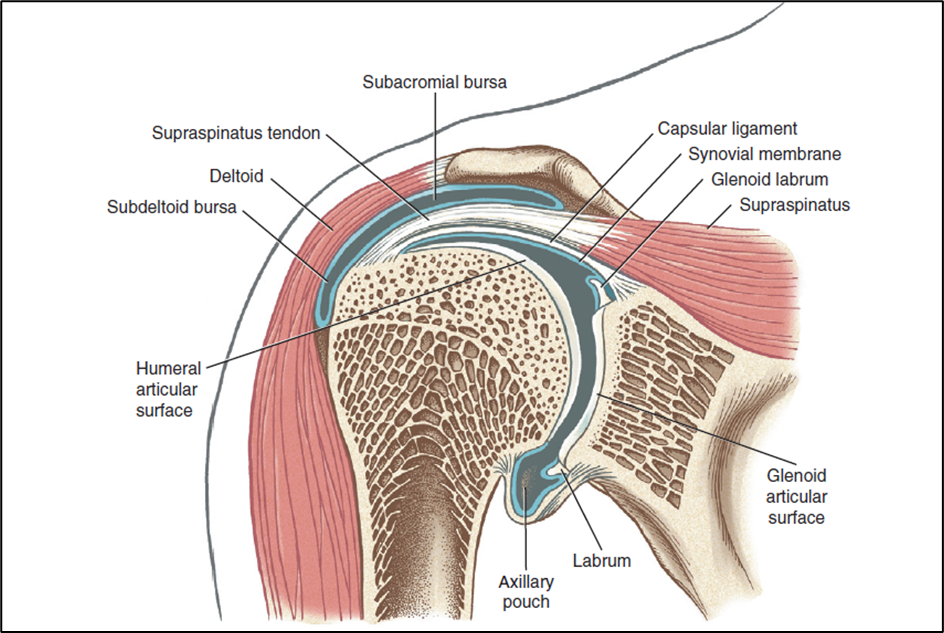
Figures 1 and 2 below show the soft tissues present around the shoulder. (Images taken from Magee, David J. (2014). Orthopedic Physical Assessment (6th. Ed). St. Louis, Missouri: Elsevier Saunders.)

Acromioclavicular joint (AC joint injuries)
The acromioclavicular (or AC joint) is a joint that connects the clavicle (collarbone) to the acromion (a bony projection on the top of the shoulder blade). It is a gliding joint that allows the shoulder blade to move up and down.
Acromioclavicular injuries are found to be the most common shoulder injury in rugby players.
Mechanism of injury
Most common mechanism of injury is a direct fall on the shoulder, especially with the area above the shoulder blade striking the ground first. This causes a dislocation of the AC joint as the ligaments that keep the joint in place get torn by the impact.
Symptoms
Pain, limited motion in the shoulder, swelling, bruising, tenderness at the top of the shoulder.

Rotator cuffThe rotator cuff is a group of muscles and tendons that attach the shoulder blade to the upper arm b More injuries
Rotator cuff injuries encompass a range of severity, from mild cuff contusions to partial and full thickness tears and can all occur in players. Rotator cuff tendinitis is also a common issue in rugby players.
Mechanism of injury
These types of injuries are mostly sustained by a direct blow to the shoulder from direct contact with an opposing player or a fall. Usually, the mechanism of injury is an impact or less commonly, could be an ABER (abduction-external rotation) dislocation.
Symptoms
Difficulty and pain caused by raising your arm, popping, or clicking sounds or when moving your arm, shoulder weakness and struggling to lift items.

Sternoclavicular joint
The sternoclavicular joint is a joint located in the middle of the chest, between the sternum (breastbone) and the clavicle (collarbone). It allows the shoulder to move up and down, and helps to keep the shoulder in its socket. The Sternoclavicular joint is also responsible for rotated shoulder movements.
Mechanism of injury
A compressive or violent force either directly over the medial clavicle or to the posterolateral aspect of the shoulder can cause a sternoclavicular injury.
Symptoms
Bruising, pain, swelling or tenderness over the joint, a deformity where the clavicle or scapula has moved, limited range of arm motion.

Glenohumeral jointThe glenohumeral joint is a ball-and-socket synovial joint and is the most mobile joint in the human More
The glenohumeral joint is the primary shoulder joint, and is responsible for a wide range of motions. The glenohumeral joint is made up of three bones: the humerus (upper arm bone), the scapula (shoulder blade), and the clavicle (collarbone). The humerus is attached to the scapula at the shoulder joint, and the clavicle attaches to the scapula at the acromion process.
Mechanism of injury
Tackle injury is the most common cause of dislocation. The rugby player tackling are more prone to have a dislocation as opposed to the players being tackled. The five-eight position on the field are at the highest chance of enduring this injury. For all rugby players, player-to-player contact results in trauma with the elbow in an extended position forcing the shoulder to exceed the limits of the normal range of motion causing anterior shoulder dislocation. Trauma with the elbow in a flexed position and the direction of the injuring force along the longitudinal axis of the humerus causes posterior shoulder dislocation. Fall, ruck, and impact are the lesser common mechanisms of injury.
Symptoms
A visibly deformed shoulder, inability to move your shoulder joint, excruciating pain, swelling, and tingling sensation from your neck that can radiate to your arms.

Superior labrum anterior-to-posterior lesion (SLAP) tears
The superior labrum is a cartilage that attaches the shoulder blade to the humerus (upper arm bone). It helps to keep the shoulder in its socket and allows for a wide range of movement. The superior labrum can be injured in a number of ways, including a direct blow to the shoulder.
Superior labrum anterior to posterior (SLAP) tears are the most common labral tears in rugby players.
Mechanism of injury
The typical mechanism of injury is usually a direct blow, consisting of a tackle where the shoulder is driven into an opposing player or, more commonly, landing on the ground directly onto the adducted shoulder while holding the ball or an opponent. Less commonly, an injury can occur if the arm is in an abducted internally rotated position for a tackle, with a direct blow to the upper arm, forcing the arm into hyperextension and internal rotation.
Symptoms
Shoulder painShoulder pain is any pain felt around in and around the shoulder joint. The shoulder is the most mob More along with mechanical symptoms such as locking, catching, popping, or snapping in the shoulder.
Biceps tendon injury
The bicep tendon attaches the bicep muscle to the shoulder blade. The bicep muscle is responsible for bending the arm at the elbow, and the bicep tendon helps to keep the muscle in place.
Mechanism of injury
Traction forces on a flexed elbow can cause injuries to the long head of biceps.
Symptoms
Swelling in the front of the elbow, bruising in the elbow and forearm, weakness in bending the elbow, weakness in twisting the forearm (supination).

Fractures
Fractures are a minority injury type in rugby players. However, upper limb fractures are more common than lower limb fractures in rugby players.
Mechanism of injury
Most commonly, a tackle injury causes a fracture. The clavicle (collar bone), proximal humerus, scapula (shoulder blade) are most commonly fractured.
Symptoms
Pain, swelling, discolouration at the site of the fracture.
Brachial plexus traction lesion
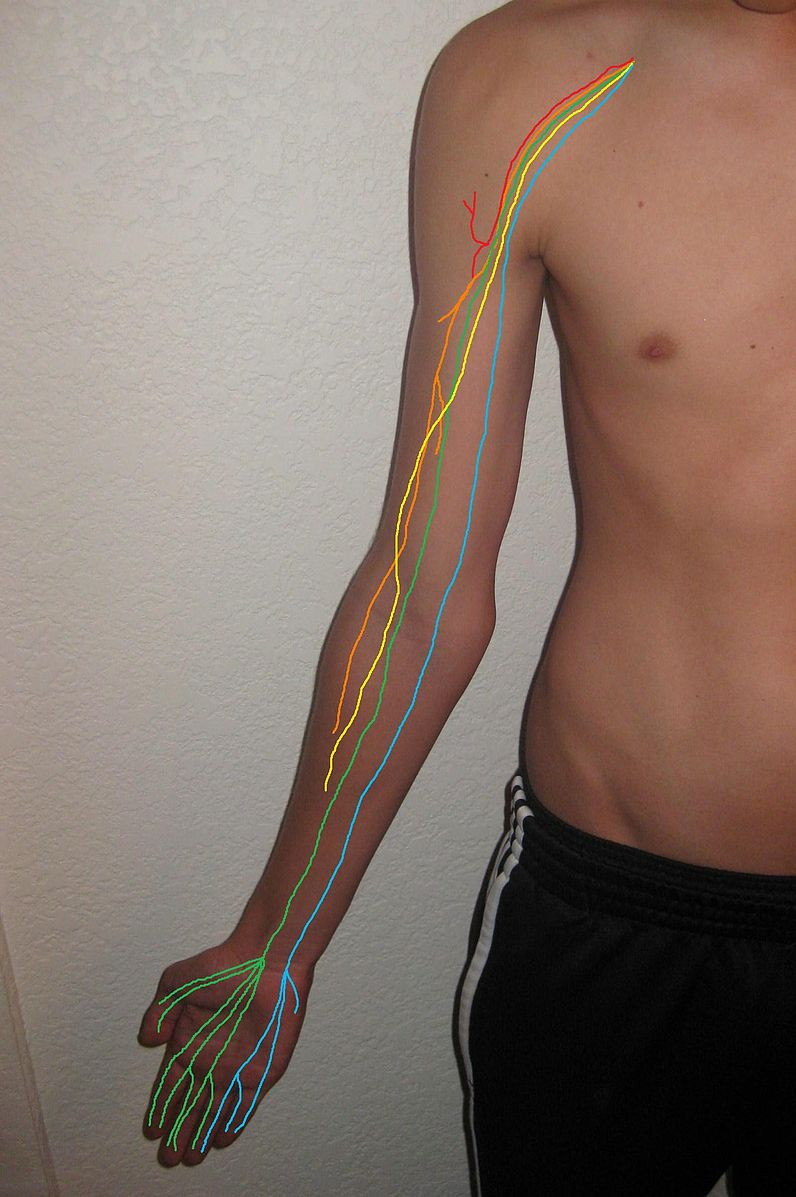
The brachial plexus is a network of nerves that runs from the neck to the arm. It controls the movement and sensation in the arm and hand.
The Brachial plexus traction lesion is a type of shoulder injury that occurs when the nerves that run from the neck to the arm are damaged. This injury is often caused by a direct blow to the shoulder, such as in a rugby tackle.
Mechanism of injury
Traction and/or compression forces acting on the brachial plexus are the primary means of injury, with traction accounting for 95% of injuries. Such injuries most commonly occur in players playing the fullback position. The injuries result from a tackle causing a depression of the shoulder and lateral flexionIs an upgoing movement from the front side or the sagittal plane facilitated by the pectorals, anter More of the head to the contralateral side. Less commonly such an injury can occur from a direct compressive force onto the supraclavicular region.
Symptoms
Numbness or loss of feeling in the hand or arm, inability to control or move the shoulder, an arm that hangs limply, burning, stinging or severe and sudden pain in the shoulder or arm.
Pectoralis major tears
A rare but serious injury is a rupture of the pectoralis major muscle. Given the demands placed on the shoulders of these players, when such an injury occurs, it will usually require surgical repair, and an extended period of rehabilitationRehabilitation is the process of helping a person regain strength and function after an injury. This More before return to professional play is possible.

Mechanism of injury
A tackle that involves a relative increase in the amount of shoulder abductionIs a sideways upgoing movement in the frontal plane brought about by the supraspinatus and the mid More, a higher point of contact on the attacking player, and an initial point of contact from the defending (injured) player more distal on the arm than is usual.
Symptoms
Pain in your chest and upper arm, weakness when you push your arms out, bruising in your chest and arm, a dimpling, or pocket, just above your armpit where the tear is located.