The Shoulder Complex made simple – from Anatomy to Function
By Manasi Satalkar, Musculoskeletal Physiotherapist
If you ask me one important joint which can help you to pull through the mountains, deep waters, and beat it out of those gangsters, it would surely be the shoulder.
But what makes this joint so special?
To tell you the truth, no other joint in the human body is as versatile with the dual functions of mobility and stability. With each activity you do, whether it’s punching, pulling, or throwing, the shoulder automates a sweet spot between the stability and mobility to complete each task with precision[1,2].
So, what do you imagine if I ask you:
“what do you think the shoulder joint is made of?”
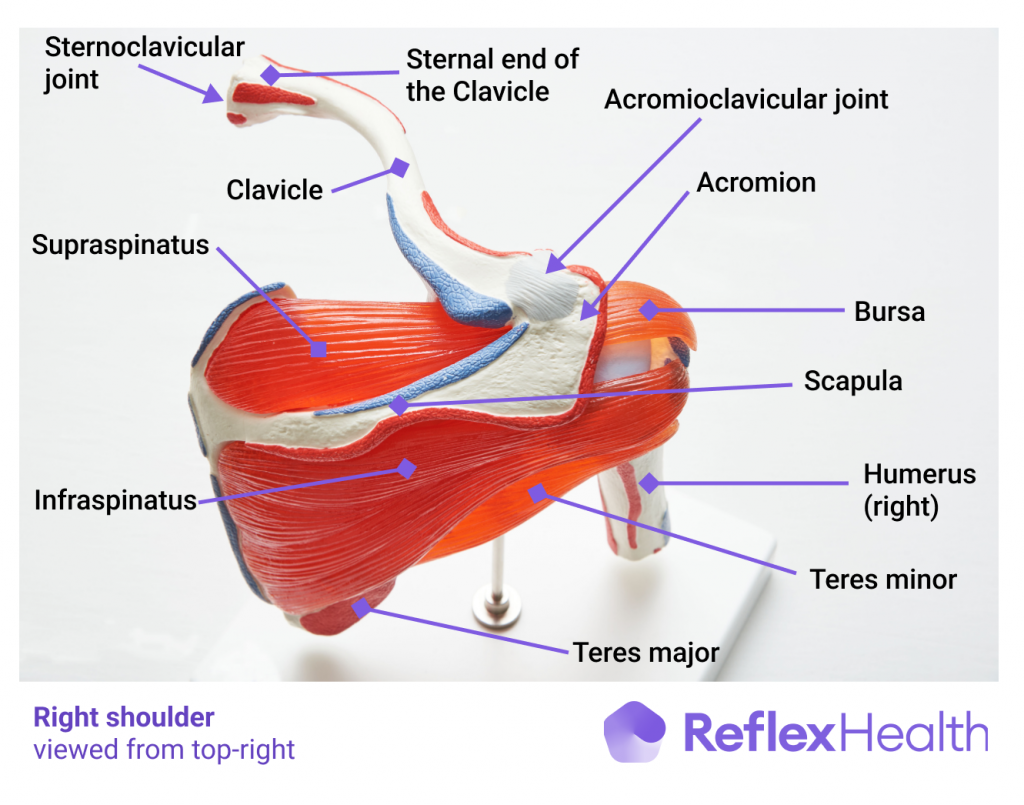
But as you imagined it is not only the ball and socket structure, rather it’s a whole complex made up of other joints such as-
1. The acromioclavicular joint, joining the scapula at the acromion to the clavicle. Also known as the AC joint
2. The sternoclavicular joint, which joins the other end of the clavicle to the sternum at the centre of the body
3. The scapulothoracic – where scapula moves on the thorax
4. The thoracic spine – the 12 vertebrae that runs from the base of the neck T1 down to the abdomen T12, and is the only part of the spine that anchors the ribcage
And of course :
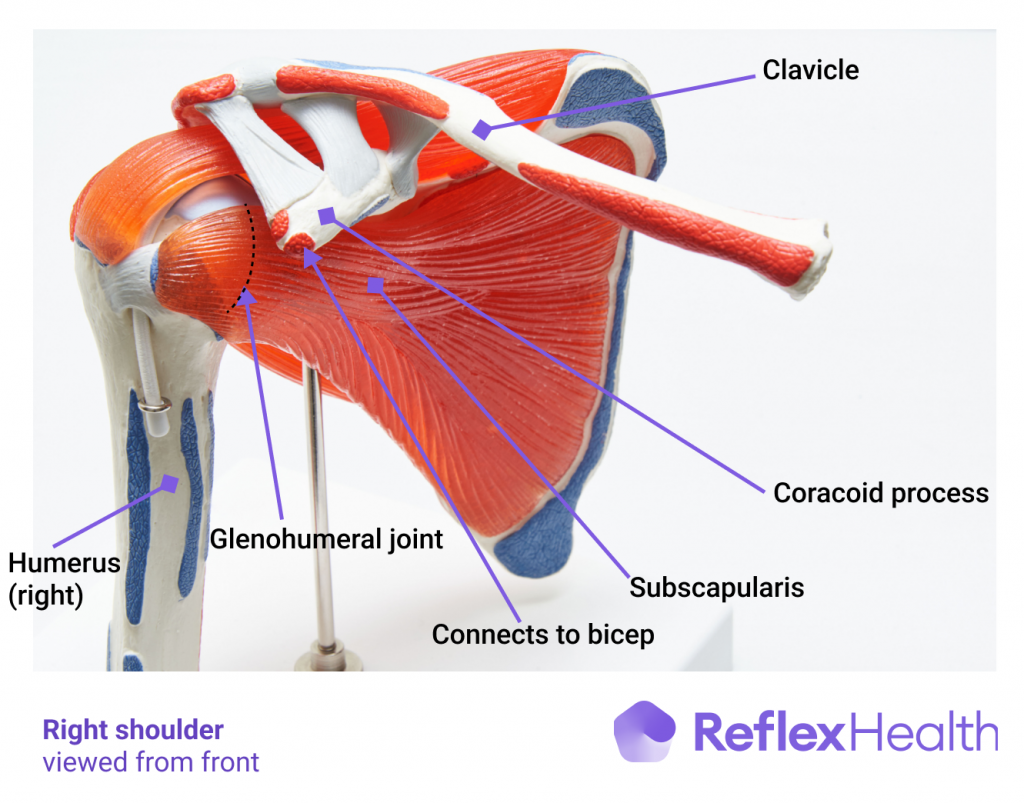
5. The ball and socket – glenohumeral joint (from Greek glene, eyeball, + -oid, ‘form of’, + Latin humerus, shoulder)
Humans as species have evolved where all these joints orchestrate together to make the movement flow into visual music which you see and get enamored by it.
Throwing to precision is the skill as Charles Darwin says humans have, due to natural selection.
No other animal can throw with velocity and power as humans do which can not only save the thrower’s life but also is a true marker of performance marvel where shoulder plays a major role [3].
Charles Darwin
To achieve this, the shoulder has anatomical benefits whose major function is to funnel down the force from the ground up and control the object’s trajectory.
So, if you ask what anatomical factors make this possible – The bony ratio of the ball that is the humeral head to the socket which is the glenoid is about 4: 1, this is like a golf ball getting ready on a golf tee [3].
This golf ball as you see is not overtly thrown in any direction thanks to the Passive or Involuntary ligaments and capsular structures surrounding the joint and The scapular – rotator cuffThe rotator cuff is a group of muscles and tendons that attach the shoulder blade to the upper arm b More muscles which stabilize it actively during the dynamic movements[4].
The rotator cuff is like the team of quality control officers of the shoulder movement – consisting of the four muscles fondly called as the SITS –
- SupraspinatusThe supraspinatus is a muscle and tendon in the shoulder that connects the Shoulder blade (scapula) More
- InfraspinatusThe infranaspinatus muscle is a large triangular shaped muscle that connects the infraspinatous foss More
- Teres MinorThe teres minor is a small narrow muscle of the rotator cuff. It works with the infraspinatus and po More
- SubscapularisSubscapularis is a muscle and tendon that connects the scapula to the front of the head of the humer More
This team works together like a stirrup to keep the ball in the socket during all the varied movements it offers which are nothing but the permutation and combinations of following basic movements [6] –
Shoulder Movements
1. Flexion
Is an upgoing movement from the front side or the sagittal plane facilitated by the pectorals, anterior deltoid, coracobrachialis and weakly by the biceps. A normal mobility of this movement which we generally refer to the range of motion is generally about 180 degrees.
2. Extension
Is a backward going movement facilitated by the Latissimus dorsi a.k.a the largest back muscle in terms of surface area, posterior deltoid and the teres major. The normal range of motion is about 45 to 60 degrees.
3. Abduction
Is a sideways upgoing movement in the frontal plane brought about by the supraspinatus and the mid deltoid. The trapezius and serratus anterior act as a force couple which spin the scapula in an upward facing socket to give shoulder an overhead mobility. Though the range of motion for abductionIs a sideways upgoing movement in the frontal plane brought about by the supraspinatus and the mid More is 180 degrees, the force couple is responsible for the range above the 90 degrees of elevation
4. Adduction
Is a frontal plane inward or towards the body coming movement brought about by the Latissimus dorsi, Pectorals and the teres major.
5. Medial rotation
Is rotatory movement along a vertical axis which can be defined as a straight line cutting your body into the right and left halves. Medial rotation brings the arm towards the body and is carried out by the subscapularis, latissimus dorsi, pectorals, teres major and the anterior deltoid. A range of motion of 70 to 90 degrees is generally the observed normal range of motion.

6. External Rotation-
Is also the rotatory movement along the vertical axis just in opposition to the external rotationThe range of shoulder external rotation is one of the most important metrics in the field of general More which brings the arm away from the body. It is one of the important components of the throwing position, which is a position of combined abduction, external rotation and a slight extensionIs a backward going movement facilitated by the Latissimus dorsi a.k.a the largest back muscle in te More. The range of shoulder external rotation is one of the important metrics in the field of general orthopedic and sports rehab, with varied conditions like frozen shoulderA condition where shoulder movement becomes very limited and painful. The cause is often unknown, bu More, rotator cuff injury, dislocation and so on. A functional range of motion between 90 to 100 degrees, in comparison with the normal is considered normal.
Ligaments of the shoulder
They not only are the packaging structures which get tightened and slack with the movements but also act as a sensor laden thickening of the capsules to inform the brain where the shoulder is positioned.
The major ligaments of shoulder are –
- The coracohumeral ligament
- The glenohumeral ligaments – which are a composite of three – the superior or the above one, the middle and the inferior glenohumeral ligaments. These attach the glenoid to the humerus and keep the ball intact in the socket.
- The coracoclavicular ligament- serving as functional link of joining the scapula to the clavicle to help the clavicle in bringing about the extra scapular range of motion[6].
If we see now the shoulder complex with so many attachments seems like an engine which would surely need some lubrication, this is brought about by the “ bursae”, fluid filled bags which helps in keeping the movement frictionless and smooth. The shoulder complex has three important bursae’s namely –
- The Subdeltoid/Subacromial bursa
- The Supraacromial bursa
- The Subcoracoid bursa
- The Subscapular recess – which is not a separate bursa but an extension of the ball and socket jointThe glenohumeral joint is a ball-and-socket synovial joint and is the most mobile joint in the human More .
- The Scapulothoracic bursae – A total number of six bursae are there out of which two are primary and the remaining four are varied and not found in all [3].
The Scapula plays a major role to take the ball and socket in an overhead position, it syncs it’s movement with it to bring in the extra stability and mobility in the overhead position
The scapula can –
1. Rotate Upwards and downwards during the abduction and adduction
2. Protract and retract with flexionIs an upgoing movement from the front side or the sagittal plane facilitated by the pectorals, anter More and extension
3. Tilt forward and backward with any upgoing and downgoing movements [4]
The Thoracic spine, which is usually in a slightly bent position, extends to facilitate the smooth overhead movement of the scapula and ultimately the whole upper extremity in the air.
So now as we see the shoulder the king of rotatory range of motion does not function in silos but is simplistically designed complex doing teamwork to make your everyday life and performance better[5,6].
Therefore, in case you feel your shoulder is not doing well, do assess each player of the team, check their metrics and try to improve each of them to bring a perceptible difference in the larger picture.
References
- Veeger HE, Van Der Helm FC. Shoulder function: the perfect compromise between mobility and stability. Journal of biomechanics. 2007 Jan 1;40(10):2119-29.
- Patel RM, Gelber JD, Schickendantz MS. The weight-bearing shoulder. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2018 Jan 1;26(1):3-13.
- Bain GI, Itoi E, Di Giacomo G, Sugaya H, editors. Normal and pathological anatomy of the shoulder. Springer; 2015 May 5.
- Neumann DA. Kinesiology of the musculoskeletal system-e-book: foundations for rehabilitationRehabilitation is the process of helping a person regain strength and function after an injury. This More. Elsevier Health Sciences; 2016 Nov 3.
- Kuhn JE. Throwing, the Shoulder, and Human Evolution. American Journal of Orthopedics (Belle Mead, NJ). 2016 Mar 1;45(3):110-4.
- Chang LR, Anand P, Varacallo M. Anatomy, Shoulder and Upper Limb, Glenohumeral Joint. [Updated 2021 Aug 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537018/