Posterior Shoulder Dislocations happen when the head of the humerus is pushed backwards, displacing it from the shoulder jointThe glenohumeral joint is a ball-and-socket synovial joint and is the most mobile joint in the human More. Posterior shoulder dislocations account for <4% of all shoulder dislocations.
What is a Dislocation?
Dislocation is defined as the complete separation of the two articulating surfaces of a joint.
What is a Posterior Dislocation of the Shoulder?
Posterior dislocation is defined when the head of the humerus is separated from the glenoid and pushed posteriorly. One of the most missed or the late diagnosed dislocation of the shoulder is the posterior one(1).
This is because the shoulder complex is guarded posteriorly by the scapula and a thick musculature covering it. This makes the posterior dislocation less frequent with about 2 -5% of the occurrence, compared to the anterior one.
About 60 – 79% of the posterior dislocations are missed during the initial examination, hence it warrants a keen examination for a good prognosis(1,2)
Aa per the basic classification, posterior dislocations can be classified as Traumatic and Atraumatic, of which the traumatic being more common.
Posterior dislocations are classified more precisely according to the etiopathogenesis and presentation as-
- Acute dislocation
- Chronic (Fixed/ Locked) dislocation
- Recurrent Posterior subluxation (more common)
Mechanism of Injury
Trauma
Trauma is the most common mechanism of posterior dislocation. 67% of all posterior dislocations occur with a high energy force directed axially to the shoulder, with the upper extremity in an internally rotated and adducted position(3).
This may be observed in the case of grabbing a dashboard during a motor vehicle collision or falling on the hand(2).
A sudden force while guarding against an opponent in combat or high-intensity sports.
Seizures
Seizures can cause posterior shoulder dislocations. In fact, 31% of the dislocations reported were being accountable due to the seizures of all the posterior dislocations(3).
A seizure is characterised by a sudden onset of high-intensity muscle contraction.
This can cause the larger muscle mass of internal rotators, consisting of the subscapularisSubscapularis is a muscle and tendon that connects the scapula to the front of the head of the humer More, latissimus dorsi, and pectorals to overpower the external rotators mainly consisting of the rotator cuffThe rotator cuff is a group of muscles and tendons that attach the shoulder blade to the upper arm b More muscles to posteriorly dislocate the shoulder.
Electrocution
A sudden passage of electric current has an incidence of 2% of total posterior dislocations (3).
Posterior Instability / Microtrauma
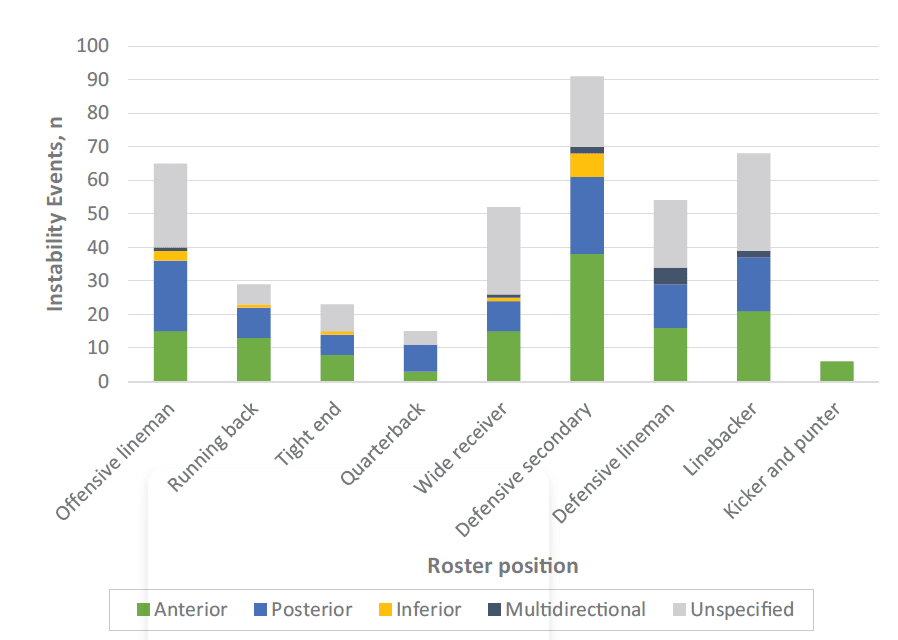
The posterior structures of the shoulder are under tension due to repeated episodes of loading. This can be seen in line backs in American Football, goalkeepers, weightlifters, and overhead athletes who repeatedly are subjected to posteriorly directed force (3,5). A recent study on shoulder instability in the NFL has shown a greater incidence of posterior instability in quarterbacks and linebackers compared to other instabilities(8). The mechanism of this can be explained as the structures getting stretched. This is seen as a continuum in fact a posterior instability gives rise to frank dislocation during the season, and hence preseason screening – prevention strategies can help in managing the injuries better.
Anterior vs Posterior Shoulder Dislocation:
The differences between anterior and posterior shoulder dislocations are shown in this table:
| ANTERIOR | POSTERIOR | |
| Position of the Humeral head | In front and inferior to glenoid | Backwards and inferior to glenoid |
| Mechanism of Trauma | Anteriorly directed force with the arm is externally rotated and abducted position | Posteriorly directed force with the arm is internally rotated and adducted position |
| Clinical Presentation |
|
|
| ASSOCIATED BONY AND LABRAL LESIONS |
|
1. Posterior Capsulolabral injury, when the posterior- inferior labrum is injured and concealed is called Kim’s lesion.
2. The bony impaction and compression fracture of the anteromedial humeral head (Hill Sach’s Lesion” 3. Associated with fracture of neck of humerus, sometimes tuberosities, and rotator cuff tears mostly in elderly(6,7). |
| Diagnostic X-ray views |
|
|
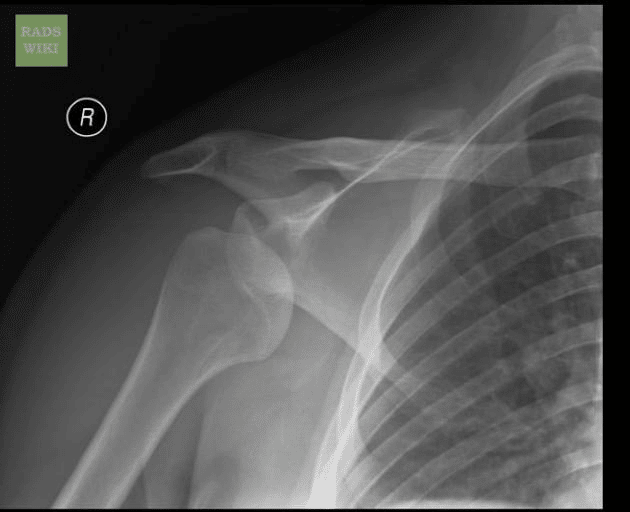
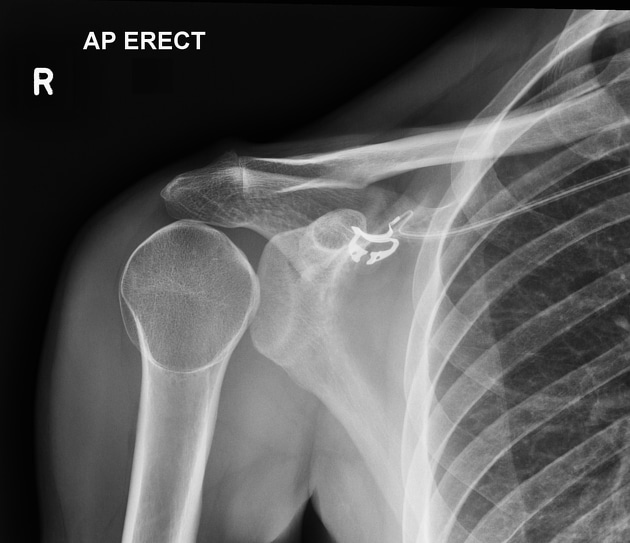
Shoulder Dislocation X-Ray
The images below show X-Rays of anterior and posterior shoulder dislocations.


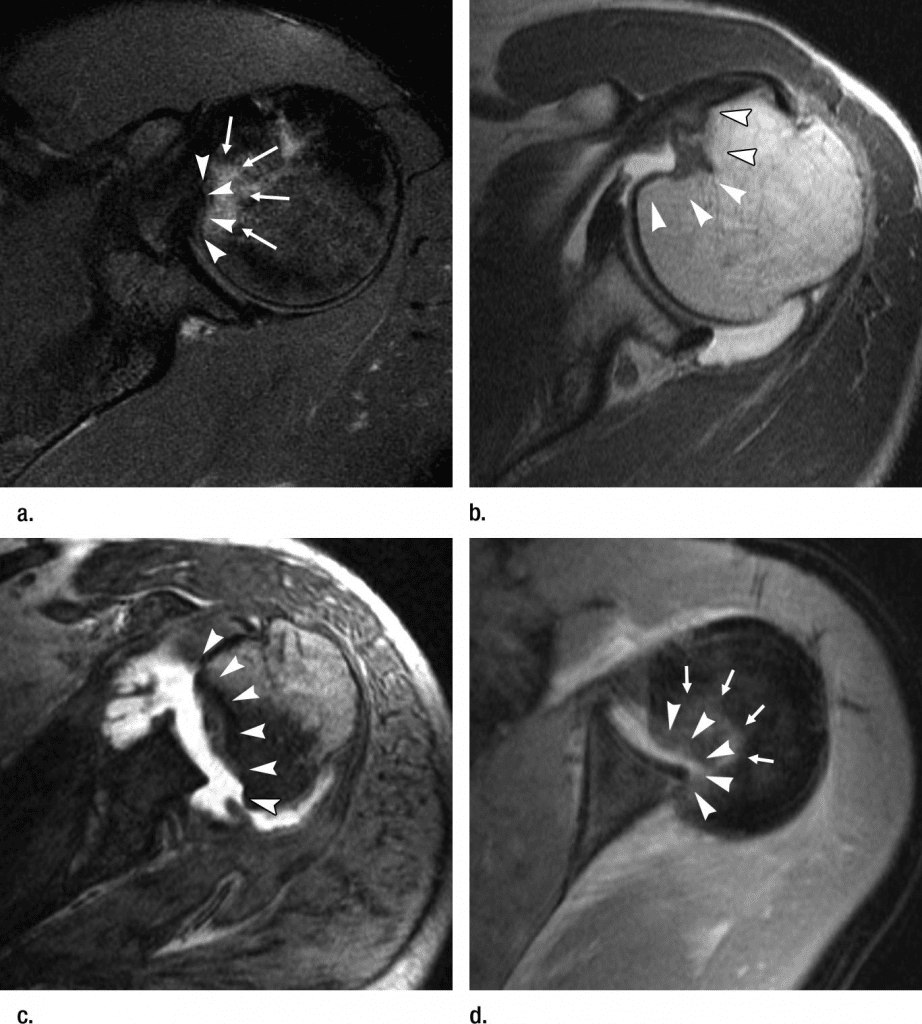
Posterior Shoulder Dislocation MRI
MRI helps in diagnosing the associated soft-tissue injuries like rotator cuff tears , bicep tendon inflammation, extent of reverse hill sach lesion and vascular supply of the humeral head(6,7).
Hence, posterior dislocation of the shoulder, one of the trickiest shoulder instability conditions to diagnose, needs a thorough assessment, a good reason for doubt, and preventive strategies in athletic shoulders, and a series of radiology investigations.
One of the main differentials in the elderly population is frozen shoulderA condition where shoulder movement becomes very limited and painful. The cause is often unknown, bu More which can give similar signs of restriction in external rotation and abduction. If misdiagnosed as the frozen shoulder the patient loses time and the viable humeral head blood supply(1). Even reduction in more than 3 weeks old chronic cases should be only taken with an in-depth investigation and consultation with a shoulder surgeon.
REFERENCES
- Perron AD, Jones RL. Posterior shoulder dislocation: avoiding a missed diagnosis. The American journal of emergency medicine. 2000 Mar 1;18(2):189-91.
- Paul J, Buchmann S, Beitzel K, Solovyova O, Imhoff AB. Posterior shoulder dislocation: systematic review and treatment algorithm. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2011 Nov 1;27(11):1562-72.
- Robinson CM, Seah M, Akhtar MA. The epidemiology, risk of recurrence, and functional outcome after an acute traumatic posterior dislocation of the shoulder. JBJS. 2011 Sep 7;93(17):1605-13.
- Rouleau DM, Hebert-Davies J. Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. Journal of orthopaedic trauma. 2012 Apr 1;26(4):246-51.
- Tannenbaum E, Sekiya JK. Evaluation and management of posterior shoulder instability. Sports health. 2011 May;3(3):253-63.
- Basal O, Dincer R, Turk B. Locked posterior dislocation of the shoulder: A systematic review. EFORT Open Reviews. 2018 Jan 15;3(1):15
- Paparoidamis G, Iliopoulos E, Narvani AA, Levy O, Tsiridis E, Polyzois I. Posterior shoulder fracture-dislocation: A systematic review of the literature and current aspects of management. Chinese Journal of Traumatology. 2021 Jan 1;24(01):18-24.
- Anderson MJ, Mack CD, Herzog MM, Levine WN. Epidemiology of shoulder instability in the national football league. Orthopaedic Journal of Sports Medicine. 2021 Apr 27;9(5):23259671211007743.
- Chan O, editor. ABC of emergency radiology. John Wiley & Sons; 2012 Dec 12.
- https://www.ortho-teaching.feinberg.northwestern.edu/XRreading/shoulder/yview.html
- Abrams R, Akbarnia H. Shoulder dislocations overview. InStatPearls [Internet] 2021 Aug 13. StatPearls Publishing.
- https://radiopaedia.org/articles/posterior-shoulder-dislocation